Please find below my opposition to the LEGALLY BINDING WHO CA+ International Pandemic Treaty.
I have found that the World Health Organization’s (WHO’s) “Zero Draft” the new agreement on pandemic prevention, preparedness, and response, called WHO CA+, is significantly flawed. Due to the evidence and information provided below I oppose the WHO CA+ Treaty.
(1)WHO failed miserably in preventing the spread of COVID-19, the WHO CA+ draft would dramatically expand WHO authority to declare a pandemic and, thereby, trigger provisions in the treaty that would re-allocate resources and encourage governments to waive intellectual property rights
(2)New Zealand is already playing an active part in planning the WHO CA+ without consultation of the public of New Zealand’s input. The Government have been deliberately non-transparent as to the WHO CA+ and its purposes, aims, goals as to its intention as to the WHO Pandemic Treaty (Accord)
(3)The proposed Treaty is due to be introduced at the 77th World Health Assembly in May 2024. If New Zealand agrees and are compliant to the WHO CA+ this will risk further increased significant tax payer payments as to the allocation to the added expenditure it will cost our country
(4)The World Health Organization has already miserably failed since the pandemic first evolved on many accounts, yet it appears that members of the New Zealand Government are supporting and even promoting the WHO CA+ International Pandemic Treaty (Accord)
(5)The draft of the WHO CA+ clearly focuses on significantly strengthening, expanding the powers of the World Health Organization which I note signed a ‘Partnership Memorandum with the World Economic Forum on 13th June 2019.
(6)The WHO/ WEF is now a Public-Private Partnership. The UN was never originally declared as such when it was created. Obviously through the extraordinary super powers awarded to the WHO would also reward the Multi-stakeholder Corporations that WEF represents., therefore there is a massive conflict of interest that would effectively bring multistakeholder corporations, and those represented by the WEF huge wealth and power in the realms of global politics and economies. The WEF is the whisperer in the ears of the WHO.
(7)The ZERO draft of the International Pandemic Treaty focuses on hugely expanding the authority, powers of World Health Organization, which give WHO the super powers to trample on ‘intellectual property rights’ and the redistribution of knowledge and technology. The WHO will become the only one, so called source of ‘Truth’, therefore having the ability to shut down the ‘True’ source of Truth., this is very dangerous.
(8)WHO International Health Regulations 2005 failed miserably when it came to accessing China’s part in the origins of the COVID19 pandemic instead of holding them to account and responsible for their failings under the IHR2005 the WHO now parrots the CCP and even praises the Chinese regime. Therefore cannot be trusted to be such a superior force of authority over all UN Nation States.
(9)In accordance with the Charter of the United Nations and the principles of International Laws the people of New Zealand have the right to self-determine and manage their own autonomous approach to public health. This is a ‘sovereign’ right, the people of New Zealand are the ‘sovereignty who have that right. The global superior authoritative right does not lay with the WHO to control, cause damage to society, business, infrastructure or medical, technical determinations of the people of New Zealand. The people rights in New Zealand are that of ‘self determination’
(10)The people of New Zealand have in accordance with the Charter of the United Nations and the Principles of International Law the sovereign right to determine, manage their own approach to public health, this notably also means ‘pandemic prevention, preparedness, response and recovery of health systems pursuant to the autonomy of domestic policies, legislations. That is provided that within this domestic jurisdiction the control awarded to the state through the vote of the people in New Zealand ‘causes no harm, damage to the peoples of New Zealand’.
‘(11)Sadly I say there has been much damage done to the peoples of New Zealand through the governments misinformation as to the COVID19 immunizations and the mandating of these. The closures of businesses throughout New Zealand and the loss of work and income. Also the closure of schools where many children have not returned back to school.
(12)The members of New Zealand House of Representatives have shown themselves to be non-transparency upon publicly exposing the serious harms and deaths of post COVID 19 immunizations. The many law abiding decent people of New Zealand have been deliberately abused by members of the New Zealand mainstream news media that has been paid for by the Governments Journalist Fund.
(13) A member of Parliament namely Michael Wood character assassinating, labelling people those who are grieved through loss of work and income, loss of businesses as a so called ‘River of Filth’. Amongst those people he called a ‘River of Filth’ and ‘Anti -Vaxers’ were those that had been vaxed and were suffering serious harms post immunization. As noted, not one member of Parliament has apologised for this cruel emotional harm caused to people of New Zealand by members of the House of Representatives.
(14)The mandating of COVID19 Immunization. The following term has often been quoted by members of WHO and WEF, and even members of NZ House of Representatives ‘No-one is safe until everyone is Safe’. Pfizer Chief Executive has publicly admitted that they did not test their COVID19 immunization for transmission prior to entering the global market place. Evidence has shown us that those that have been injected with the Pfizer mRNA Injection have still been infected by the virus.. . Obviously the people of New Zealand have been misled when it has come to mandating of COVID19 immunizations and mandates
(15)It is a huge concern that large Pharmaceutical companies such as Pfizer have and continue to advise the Intergovernmental working group on the WHO CA+ International Pandemic Treaty as to the Zero Draft which is a huge conflict of interest.
(16)It is a deep concern that if the New Zealand Government continues to pursue, support the WHO CA+ International Pandemic Treaty (Accord) it would give the WHO superior authority over NZ Domestic policies. WHO would have the power to declare a pandemic globally whether New Zealand is affected or not and could have the power to reallocate resources.
(17)The Zero Draft of the WHO CA + Pandemic Treaty makes transparency and cooperation mandatory (legally Binding). Uses the word ‘shall’ when referencing facilitating accessing, sharing of research and genomic data, however there are no repercussions for ‘non-compliance’. It is evidently clear that the WHO and those drafting this treaty , and those that support, promote it have learned nothing. There is no reason to believe that China would be compliant with the obligations set out in the WHO CA+ International Pandemic Treaty (Accord) I also note that the World Health Organizations failure to quietly abandon investigations into China’s incompetence to comply to the legally binding WHO Health Regulations (IHR 2005)
(18)The WHO CA+ Draft lets China off the hook. Despite China having the largest economy in the world the United Nations considers China as a developing country. Developed countries financially support developing countries when it comes to ‘common but differentiated responsibilities’ among nations. Developed countries would share the greater costs therefore China will likely be the beneficiary of the WHO CA+ obligation for developed nation parties, among other provisions.
(19)The WHO CA+ Pandemic Treaty Zero Draft calls on the parties to tackle misleading, misinformation or disinformation. Yet the WHO themselves have been the source of disinformation when they tweeted “preliminary investigations conducted by the Chinese authorities have found no clear evidence of human-to-human transmission of COVID 19.
I refer to the ‘World Health Organization ‘Preliminary investigations conducted by the Chinese authorities have found no evidence of human to human transmission of the novel coronavirus (2019-n CoV) identified in Wuhan Vina. Twitter January 14th 2020 18
https://twitter.com/WHO/status/1217043229427761152
(20)As for the CDC on the efficacy of facial mask wearing that shifted over time, when Anthony Fauci defended flip flop accusations after shifting mask guidance, this has reported changed time and time again. There is much controversy about mask wearing. It is clearly evident that many people wear masks as chin straps. Masks do risk emotional, psychological damage to some extent. Mask wearing is not normalised behaviour so will affect people in different ways. LINK: Independent, July 29, 2021, https://www.independent.co.uk/news/world/americas/us-politics/fauci-cdc-mask-flip-flop-b1892600.html
(21)A recent study found that natural immunity acquired by a COVID-19 infection was “associated with lower incidence of SARS-CoV-2 infection, regardless of the variant, than mRNA primary-series vaccination. Yet WHO superior authorities under a legally binding Pandemic Treaty could mandate all populations to be vaccinated, immunized without accountability. This is very dangerous.
LINK:” Hiam Chemaitelly et al., “Protection from Previous Natural Infection Compared with mRNA Vaccination Against SARS-CoV-2 Infection and Severe COVID-19 in Qatar: A Retrospective Cohort Study,” The Lancet, November 11, 202, https://www.thelancet.com/journals/lanmic/article/PIIS2666-5247(22)00287-7/fulltext (accessed February 24, 2023).
(22)The WHO and UN Member Nation Governments and their so called experts have been proven wrong far too often, yet the WHO Pandemic Treaty gives WHO the global super power authority to police “disinformation. This seriously infringes on the internationally accepted right to freedom of expression. (UN International Human Rights and NZ Domestic Human Rights Legislations)
(23)The WHO CA+ Treaty Draft emphasizes ‘Equity’. It is guided by ‘Equity’, which is defined by the absence of unfair, unavoidable or remediable differences among and within countries, including between different groups of people, whether these groups are defined socially, economically, demographically, geographically or references ‘Inequality’. The term ‘Equity’ and ‘Equitable’ appear more that thirty times in the ZERO Draft of the Treaty, however there is no clear definition what this means.
(24)The people of New Zealand have the right to have clear, concise information. (ibid., Art 3,4 (3) ). It is evidential by the ZERO Draft of the WHO CA+ Treaty that it is guided by ‘Equity’, a term that is deeply rooted in ‘Marxist’ ideology and should never be embedded in the guiding principles of any international legally binding commitment of any State, including that of New Zealand.
(25)The ZERO Draft of the CA+ International Pandemic Treaty (Accord- Convention) commits to the term ‘Universal Health Coverage’, this is not clearly defined. I stand to be corrected, but does that mean that the Government provides the peoples of New Zealand health care, is that with or without costs to the peoples of New Zealand, and at what costs must the people of New Zealand pay?. How will this indeed affect tax payers pockets?
(26)Its obvious that if the NZ House of Representatives agree, comply to the WHO CA+ International Pandemic Treaty domestic legislations will have to be amended. The people of New Zealand are not awarded end decision making rights when it comes to domestic policy making. I refer to the (Non-Legally Binding Citizens Initiated Referenda), and even if this did become ‘Legally Binding’ the people of New Zealand would have no end decision rights when it comes to Domestic Policies due to the legally binding nature of the WHO CA+ Treaty.. Therefore upon voting for political parties at election time, this means that promises made to the voting public can be over- ridden by the WHO Pandemic Treaty
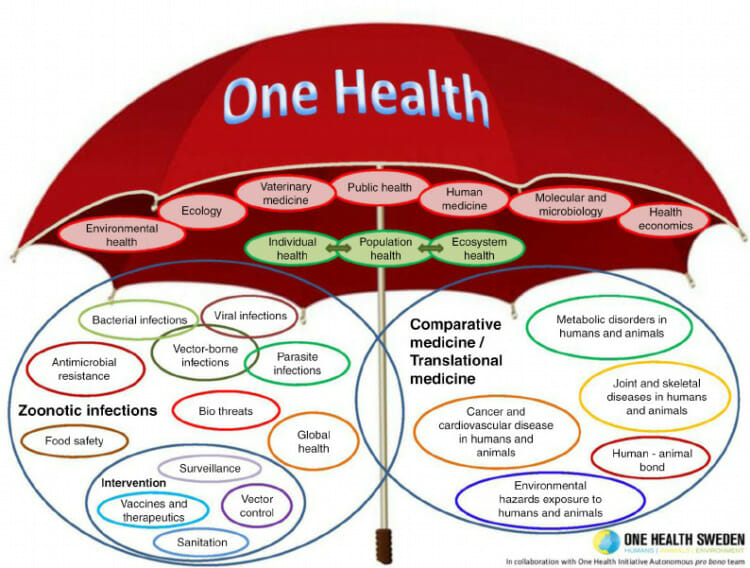
(27)The WHO CA+ Pandemic Treaty (Accord) incorporates a ‘One Health’ approach framework. This includes ‘Humans, Animals-wild and domestic and all Eco-systems’. This means that the WHO under the WHO CA+ International Pandemic Treaty has massive super superior control over every aspect of life on this planet.
(28)WHO CA+ Treaty under the classification of ‘Climate Change’ will have the authority to restrict, control food systems, trade and travel, infrastructure, land use and property rights. This is scandalous and extremely dangerous when it comes to the health and wellbeing of New Zealanders.
(29)Those that reside in the NZ House of Representatives are accountable to the people of New Zealand who voted them in to the political positions they hold in the New Zealand House of Representatives. To be responsible and accountable to ALL peoples of New Zealand. Through researched evidence of viewing speeches in the House and other UN Information that New Zealand Members of Parliament are supporting, promoting and are in agreeance with the WHO ZERO Draft of the CA +.
(30) I also note that at the 77th gathering of the World Health Assembly the final draft of the CA+ WHO International Pandemic Treaty will be produced, introduced to all UN Member Nation States to determine whether, and which UN Member States agree on the WHO International Pandemic Treaty (Accord)
(31) I therefore request that the NZ House of Representatives transparently accords the peoples of New Zealand open public debate, discussion without political intrusion as to all knowledge, information that is pertained in every ZERO draft of the WHO CA+ Pandemic Treaty as it is produced, introduced.
The draft states that the WHO CA+ “shall be subject to ratification, acceptance, approval or accession by UN Member Nation States, therefore clearly requires advice and consent under the process outlined., “Circular 175 Procedure,” https://2009-2017.state.gov/s/l/treaty/c175/index.htm (accessed February 24, 2023).
(32)I conclude that the WHO CA+ International Pandemic Treaty (Accord) is highly problematic and deeply flawed and would allow the global superior powers of the World Health Organization (UN) to have authority over New Zealand’s domestic policies. One size does not fit ALL and there is no evidence of ‘trustworthiness’ as to why the people of New Zealand should support this WHO Treaty proposal.
(33)The ‘Public-Private’ partnership of the World Economic Forum with the UN is a huge conflict of interest as they are the ‘whisperers in the ear’ of the UN, therefore also rewarded global superiority political, economical control through the WHO CA+ International Pandemic Treaty (Accord) agreeance.
Therefore, for all the above reasons , information provided I totally oppose the WHO CA+ International Pandemic Treaty (Accord). I find it to be highly dangerous to the health and wellbeing of ALL peoples of New Zealand. I have cc’d other groups, individuals, organizations, members of parliament the above information-communication t as outlined to the NZ House of Representatives as to opposition of the WHO CA+ International Pandemic Treaty.
I request a response at your earliest. Thank you.
Carol Sakey
...